Population Health Management for Frailty and Long Term Conditions
Target Health Solutions (THS) helps NHS organisations deliver population health management for people living with frailty and long term conditions.
We do this through a digital platform supporting proactive identification, risk statification, shared digital comprehensive geriatric assessment (CGA), coordinated recall systems, and clinical decision support across General Practice and Integrated Neighbourhood Teams (INTs).
This improves efficiency, workforce capacity, and financial sustainability for organisations while delivering better outcomes for people living with frailty and long term conditions.
Population Health Management for Long Term Conditions in General Practice
Population Health Management for Frailty in Integrated Neighbourhood Teams
Population Health Management for Frailty and Long Term Conditions
Examples from General Practice and integrated neighbourhood teams
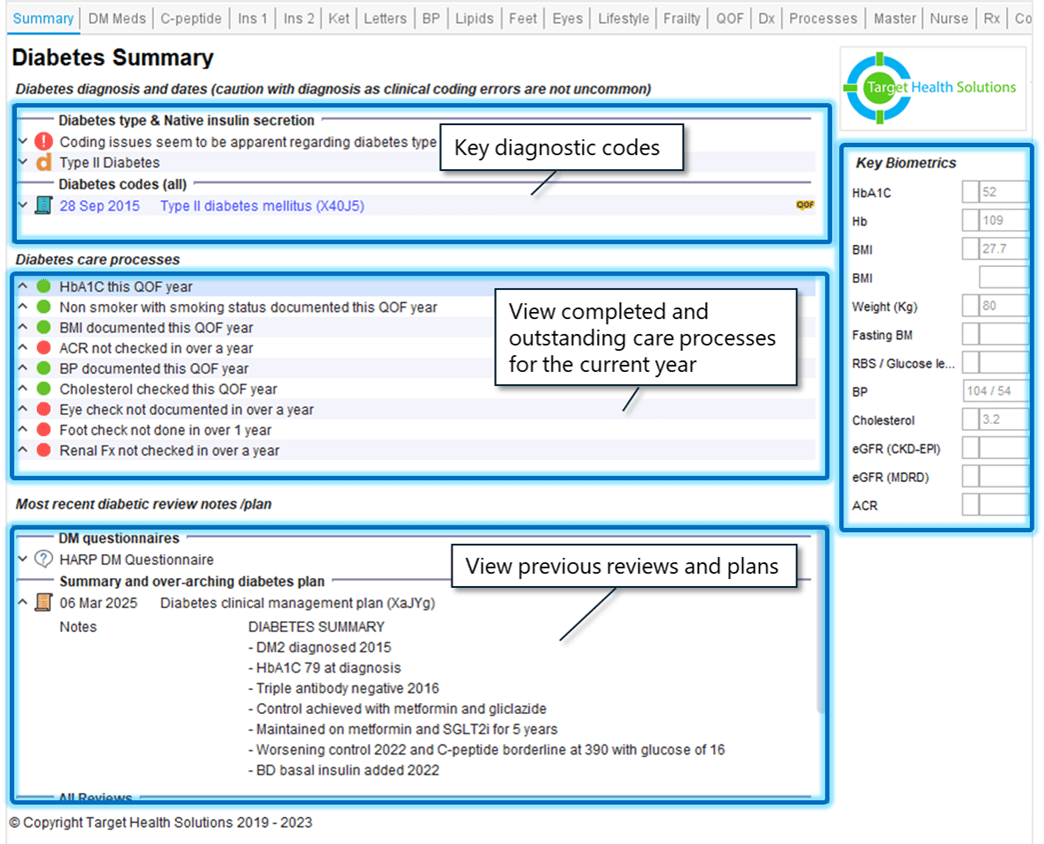
One coordinated encounter instead of multiple fragmented appointments
THS’s integrated long term condition templates bring patient history, prescribing, and secondary care data into a single clinical view, supporting safer decisions, more efficient reviews, and higher quality care.
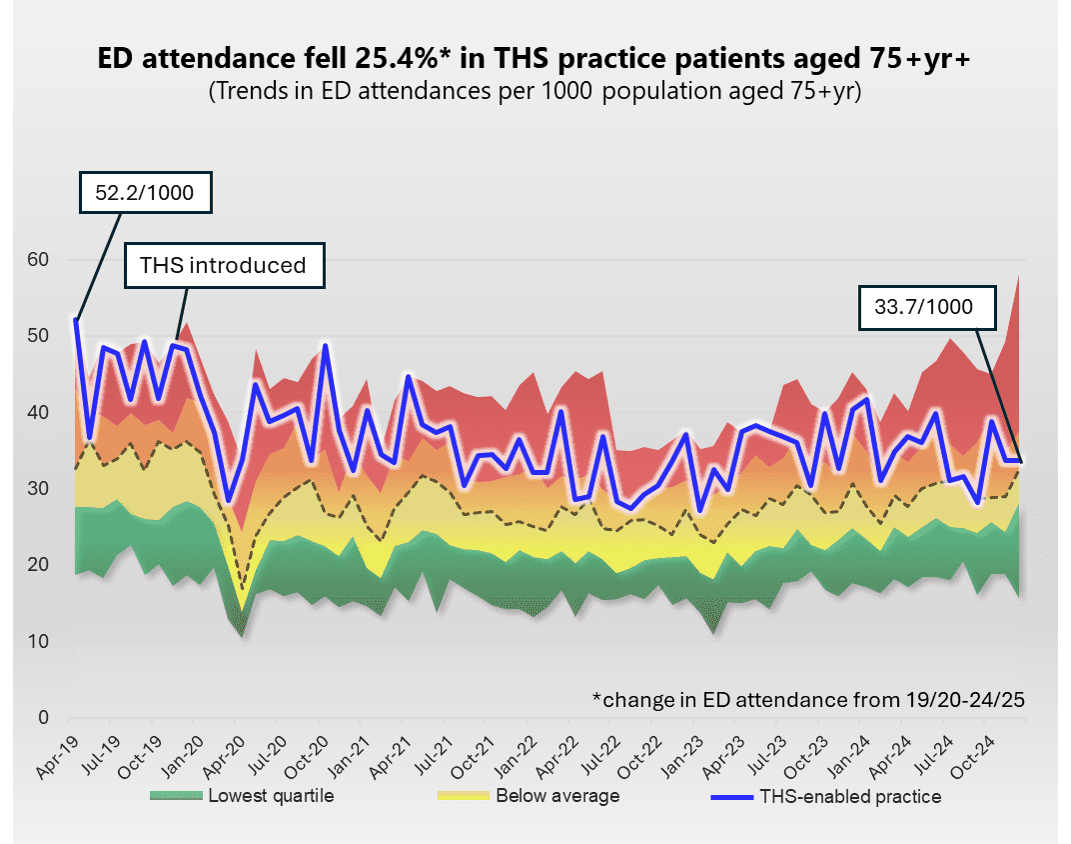
Reducing hospital admissions in frailty
THS supports population health management for frailty through software that enables:
- Earlier identification
- Risk stratification and prioritisation
- Shared digital Comprehensive Geriatric Assessment (CGA)
- Coordinated care across Integrated Neighbourhood Teams.
This helps organisations intervene earlier and support more people to remain well at home.
Smarter recall systems for long term conditions
Digital Comprehensive Geriatric Assessment (CGA) for Integrated Neighbourhood Teams
iCGA 3.0 is a digital Comprehensive Geriatric Assessment (CGA) platform that supports Integrated Neighbourhood Teams to deliver shared assessment, coordinated care planning, and continuity across organisations for older people living with frailty and dementia.
Built-in clinical alerts identify high-risk medications and poorly optimised long term conditions, supporting safer and more consistent delivery of CGA across neighbourhood teams.
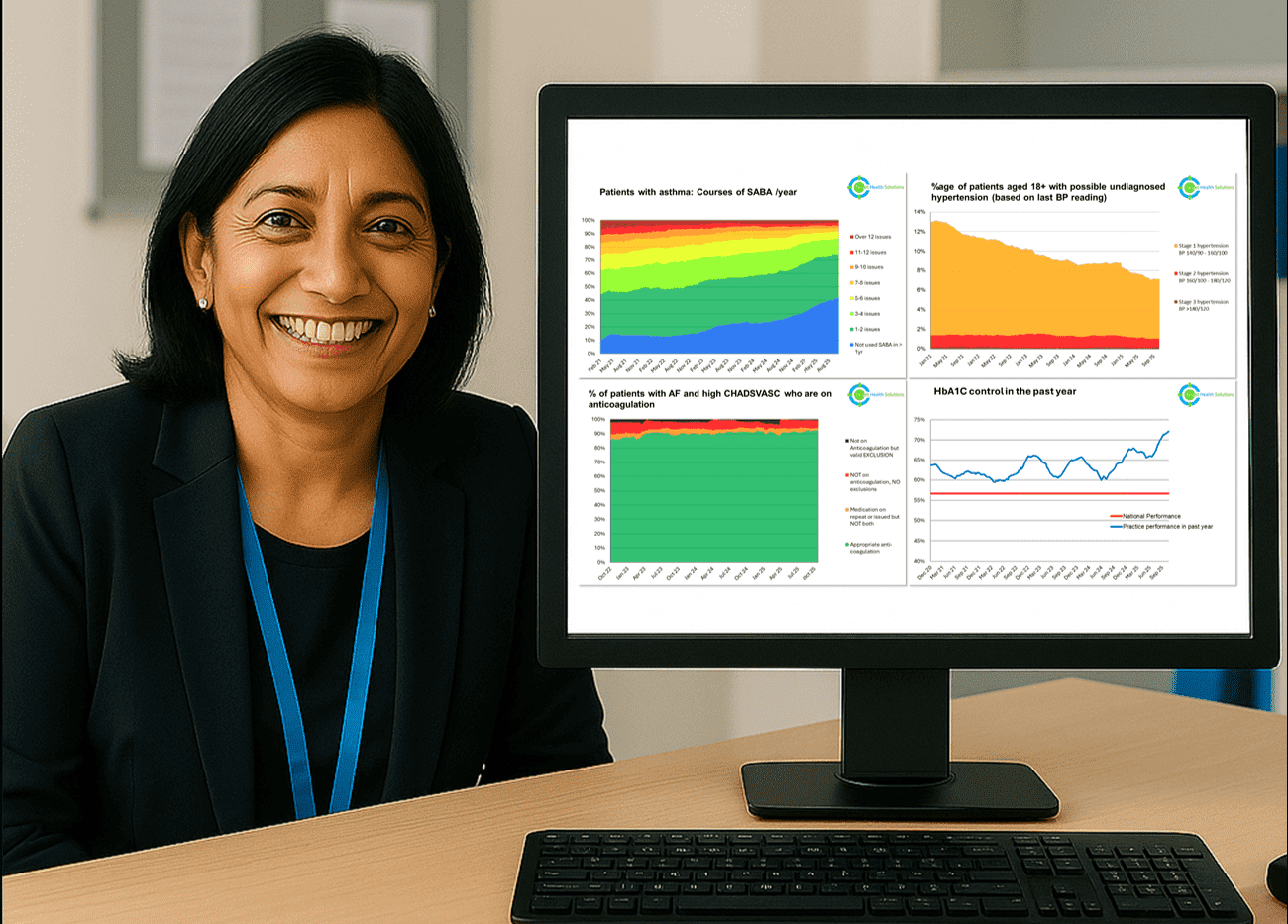
Population health management dashboards for proactive care
This helps teams identify unmet need, prioritise proactive care, and focus support on the people who need it most.
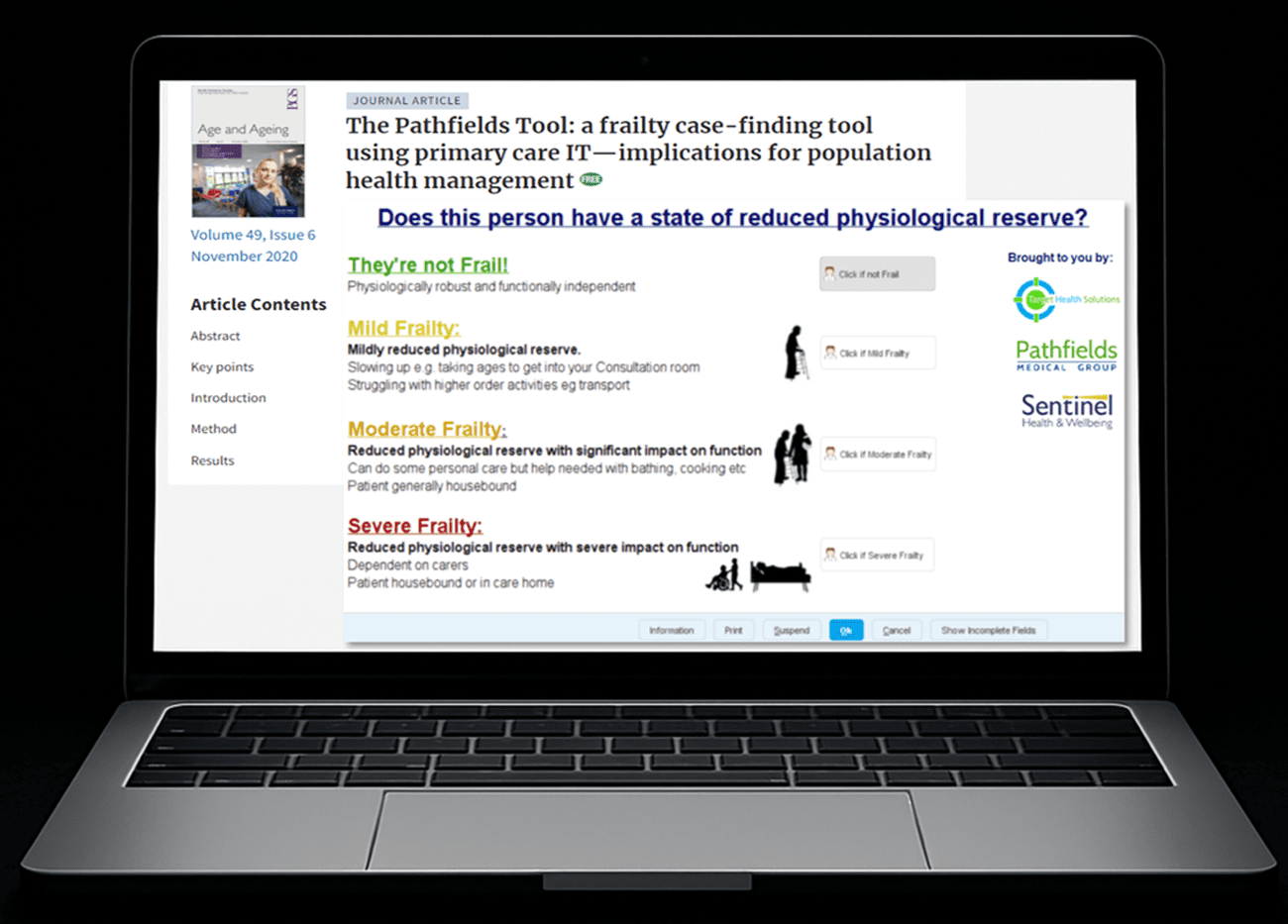
Better frailty and long term identification, backed by research
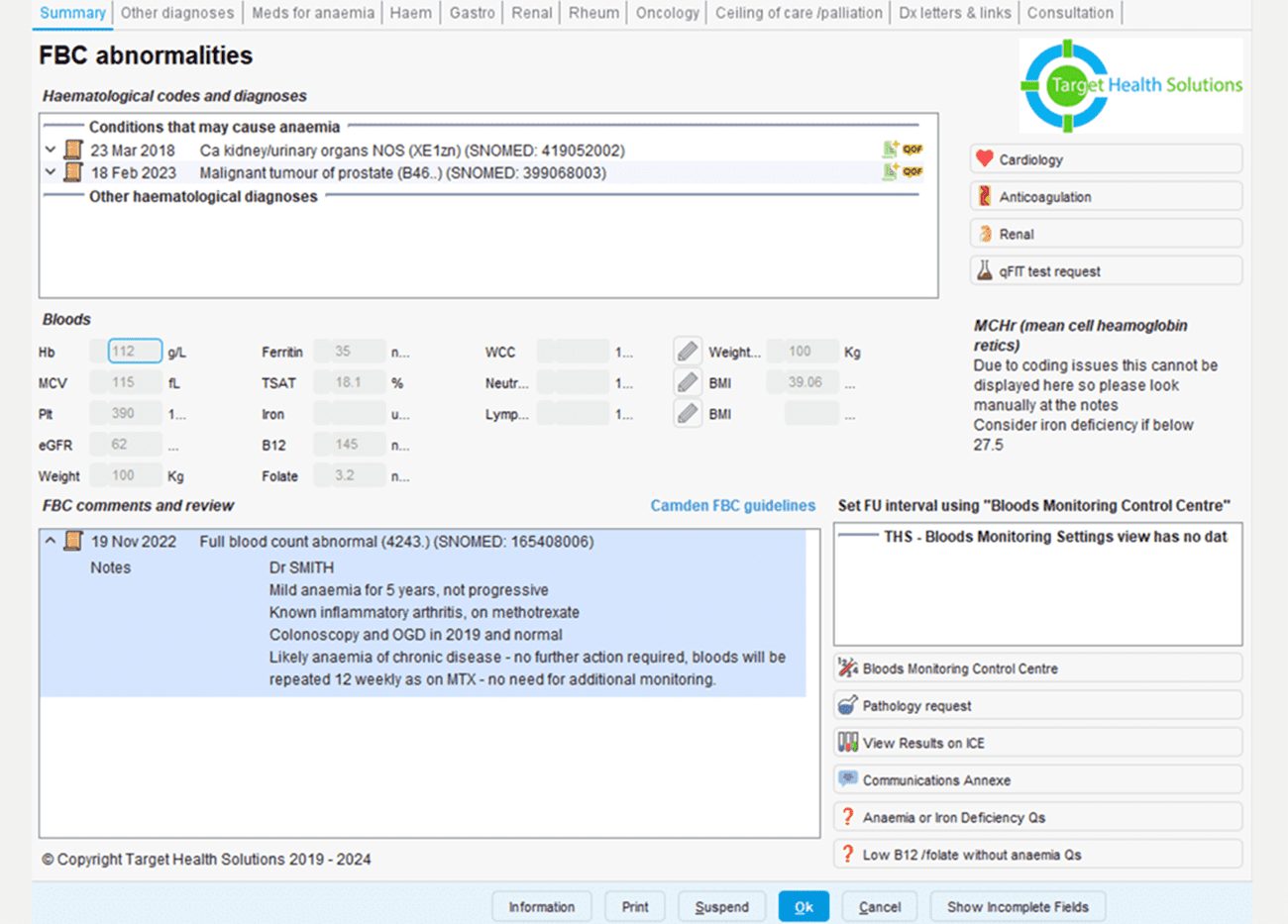
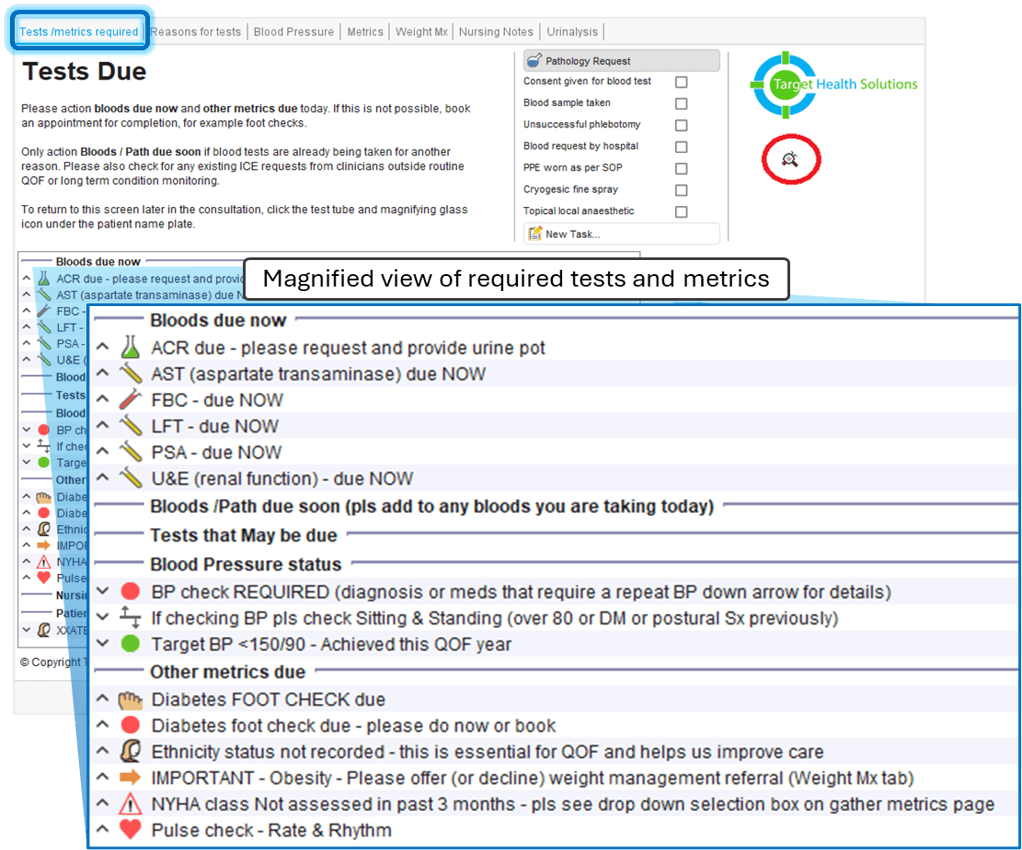
Integrated blood monitoring and results management
Clinicians can record decisions, manage follow-up, and communicate with patients from a single clinical view, supporting continuity and more efficient monitoring across general practice.
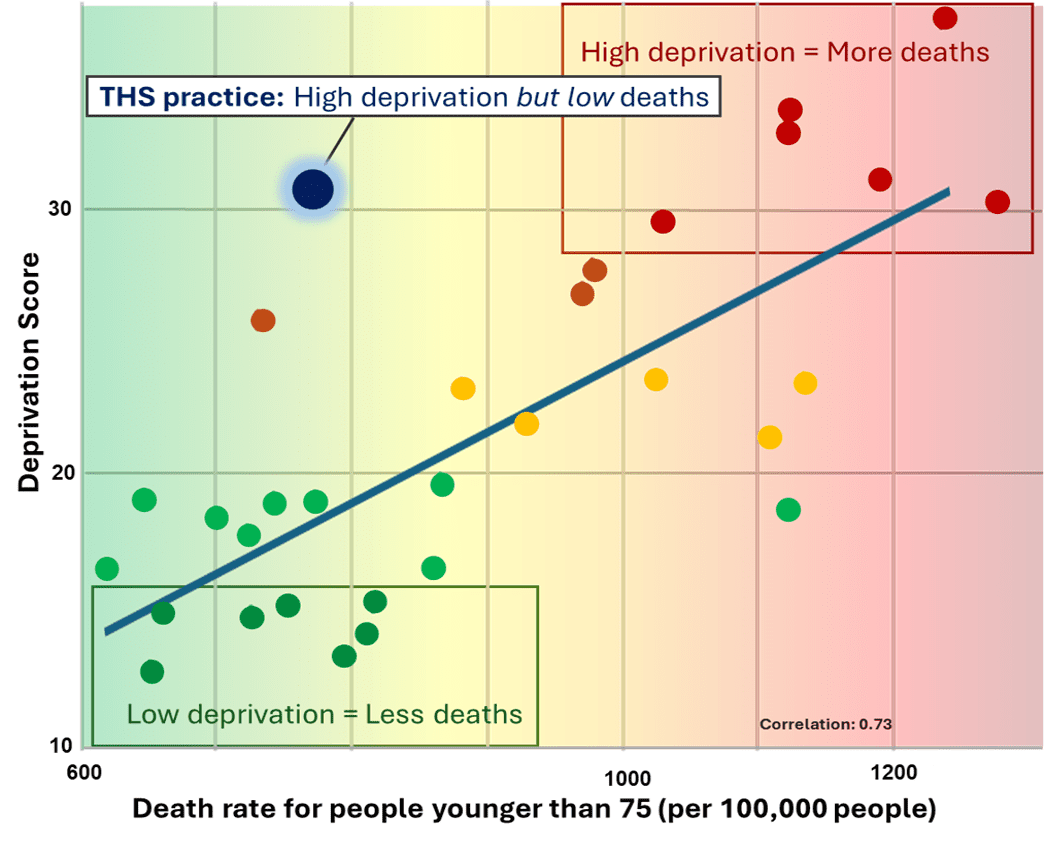
Tackling health inequalities
Contact us

