The Pathfields Tool.
Continuous frailty identification in routine care, creating a self-replenishing frailty register.
Free for NHS use.
The NHS cannot manage Frailty if it cannot see it.
Frailty identification is the entry point to population health management. It must be accurate, scalable across the whole population, enable early identification, and be simple for clinicians to use.
Accurate Frailty identification matters.
Half of all hospital beds in the UK are occupied by people aged 75 or more. Most have frailty.
Superior diagnostic accuracy
Compared with eFI 1, it identified twice as many people at high risk of frailty, with clinicians confirming frailty in 75.9%.
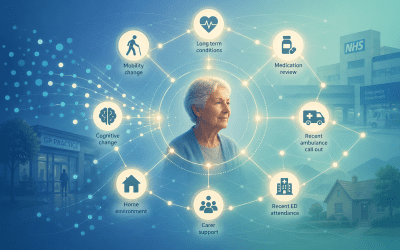
Continuous Frailty identification in routine care
Systematically identifies frailty in patients aged 65+ during routine consultations. When relevant risk factors are present, clinicians are prompted to assess and record frailty using clinical judgement. Once completed, the prompt remains inactive for 12 months to avoid alert fatigue, creating a continuously updated frailty register over time.
Identifies mild frailty
Systematic detection of mild frailty, enabling earlier intervention, slowing decline, and in some cases preventing progression altogether
Evidence based and in routine use
The Pathfields Tool has been independently peer reviewed and published and now in routine use across NHS organisations.
Time neutral
Unlike other tools, this is time neutral. Diagnosis relies on the clinician’s knowledge of the patient and two clicks of a mouse button.


The wider challenge.
Find out more about how the Pathfields Tool supports population health management of frailty, and the wider challenge it exposes: The NHS already delivers many components of effective frailty care, but they remain fragmented rather than coordinated.
Explore the Frailty Paradox series to understand why this persists, and what needs to change.

The NHS Frailty Paradox Series: Part 8 | From Digital infrastructure to population health management
The NHS already delivers many of the components of effective frailty care. In this final part of the NHS Frailty Paradox series, we explore how digital infrastructure helps overcome fragmented information and human cognitive limits, supporting identification, prioritisation, intervention, and monitoring across a frailty population.
Through practical examples, we show how digital infrastructure helps neighbourhood teams deliver population health management of frailty at scale.

The NHS Frailty Paradox Series: Part 7 | The missing foundation for neighbourhood frailty care: digital infrastructure
Population health management for frailty depends on identification, prioritisation, intervention, and monitoring. But even when neighbourhood teams are organised to deliver continuity, coordination, and Comprehensive Geriatric Assessment, two constraints remain: fragmented information and human cognitive limits.
This article explores why both undermine frailty care and why digital infrastructure has become one of the foundations of effective population health management.
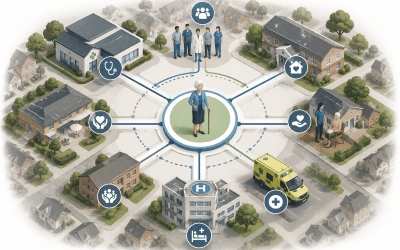
The NHS Frailty Paradox Series: Part 6 | System enablers for CGA: Why PCN hubs and neighbourhood teams matter
Frailty care is rarely limited to a single team, service, or episode of care. Effective Comprehensive Geriatric Assessment (CGA) depends on continuity and coordination across neighbourhood systems over time. This article explores how PCN Hubs, Integrated Neighbourhood Teams, and locality-wide frailty services can organise continuous CGA around people living with frailty.
The NHS Frailty Paradox Series: Part 5 | From Identification to System: Making Population Health Management Work
Population health management for frailty is not defined by identification alone, but by delivering the right intervention at the right stage of frailty progression.
Part 5 of the Frailty Paradox series explores frailty management across the spectrum, from prevention and early intervention through to Comprehensive Geriatric Assessment (CGA), continuity, and coordination for people living with moderate and severe frailty.
The NHS Frailty Paradox Series: Part 4 | When Everyone Is at Risk, Who Do You Prioritise?
Not everyone living with frailty can be seen. The question is who is reached in time.
In Part 4 of the Frailty Paradox series, we explore how signals of deterioration are used to prioritise risk and target coordinated care.

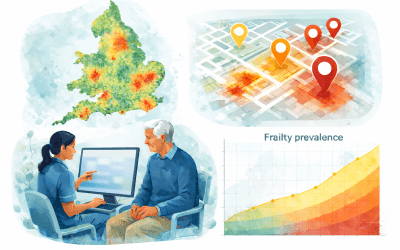
The NHS Frailty Paradox Series: Part 3 | Bridging the Gap: From Frailty Identification to a Self-Replenishing Frailty Register
Frailty identification in the NHS is often fragmented, inconsistent, and reactive.
In Part 3 of the Frailty Paradox series, we explore how continuous, clinician-led identification through a self-replenishing frailty register can make frailty visible across a population, forming the foundation for effective prioritisation and intervention.
The NHS Frailty Paradox Series: Part 2 | Frailty Identification in Integrated Neighbourhood Teams
The NHS cannot manage frailty if it cannot see it.
In Part 2 of the Frailty Paradox series, we explore why general practice is best placed to anchor a shared, system-wide view of frailty. We examine the strengths and limitations of current approaches, drawing on real-world experience and published evidence.
The findings suggest that current methods may identify fewer than half of patients living with frailty, and that no single tool meets all four key requirements for effective identification: accuracy, scalability, early detection, and usability in clinical practice.

The NHS Frailty Paradox Series: Part 1 | The Work Exists, The System Does Not.
The NHS is not failing to deliver frailty care. The workforce is already identifying risk, assessing need, and delivering support every day, but this activity is not organised as a coordinated neighbourhood response.
This is the Frailty Paradox: the work exists, but the system to bring it together does not.
This series explores how the NHS can move from fragmented activity to coordinated population health management for frailty through integrated neighbourhood teams.


Visit our sister site
Book a Demo