by David Attwood
The NHS already delivers many of the components of effective frailty care. In this final part of the NHS Frailty Paradox series, we explore how digital infrastructure helps overcome fragmented information and human cognitive limits, supporting identification, prioritisation, intervention, and monitoring across a frailty population.
Through practical examples, we show how digital infrastructure helps neighbourhood teams deliver population health management of frailty at scale.
by David Attwood
Population health management for frailty depends on identification, prioritisation, intervention, and monitoring. But even when neighbourhood teams are organised to deliver continuity, coordination, and Comprehensive Geriatric Assessment, two constraints remain: fragmented information and human cognitive limits.
This article explores why both undermine frailty care and why digital infrastructure has become one of the foundations of effective population health management.
by David Attwood
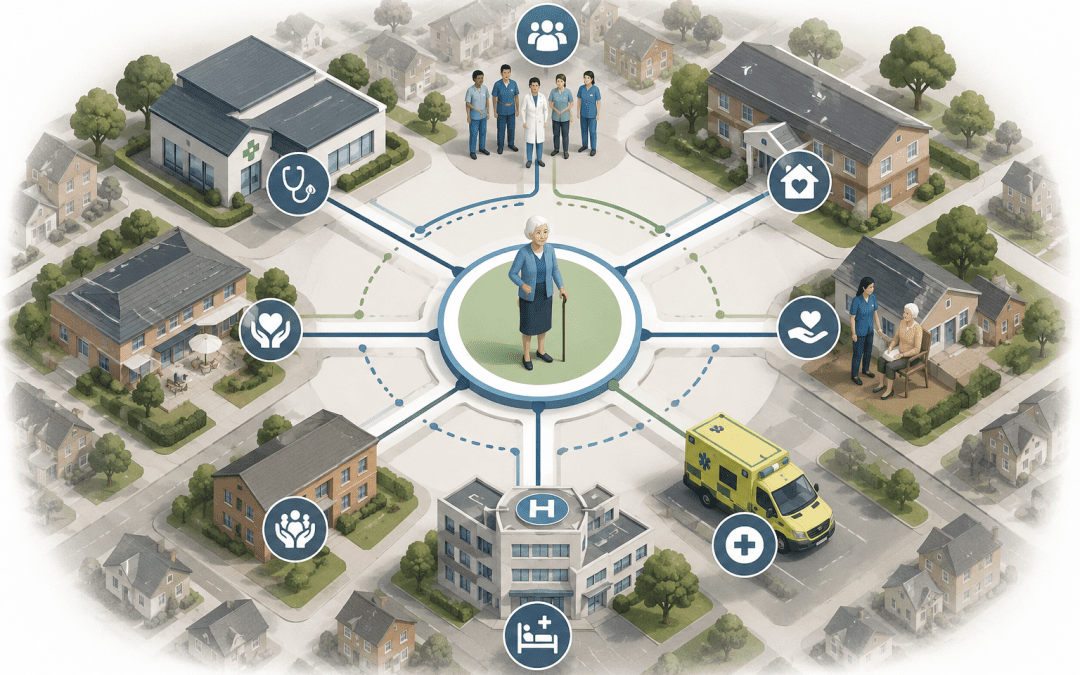
Frailty care is rarely limited to a single team, service, or episode of care. Effective Comprehensive Geriatric Assessment (CGA) depends on continuity and coordination across neighbourhood systems over time. This article explores how PCN Hubs, Integrated Neighbourhood Teams, and locality-wide frailty services can organise continuous CGA around people living with frailty.
by David Attwood
Population health management for frailty is not defined by identification alone, but by delivering the right intervention at the right stage of frailty progression.
Part 5 of the Frailty Paradox series explores frailty management across the spectrum, from prevention and early intervention through to Comprehensive Geriatric Assessment (CGA), continuity, and coordination for people living with moderate and severe frailty.
by David Attwood
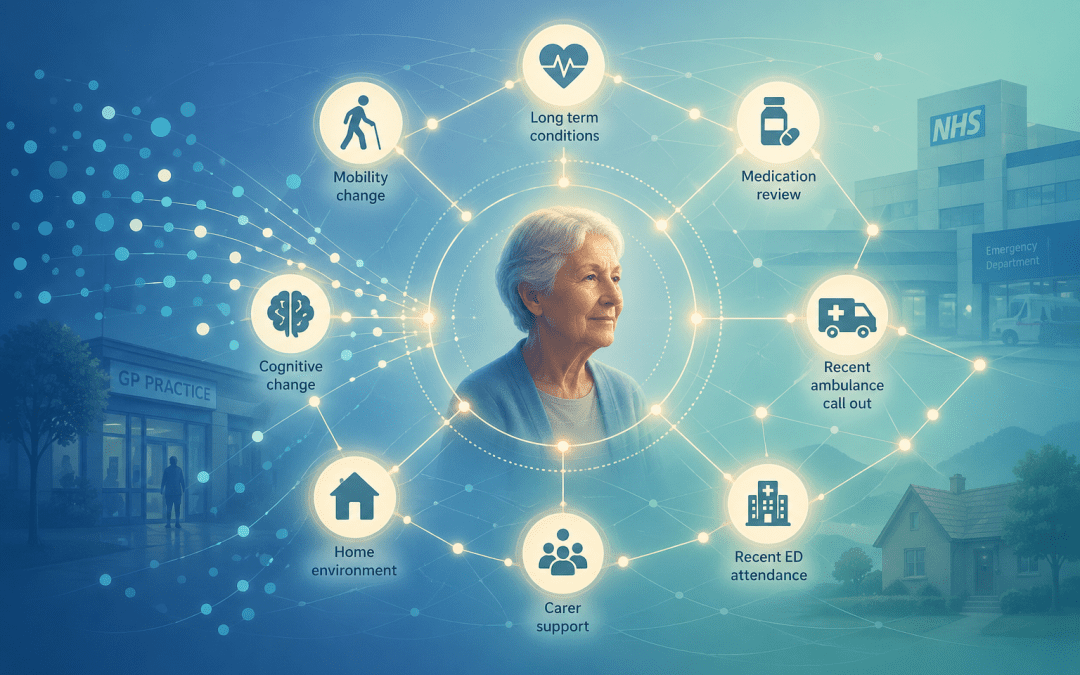
Not everyone living with frailty can be seen. The question is who is reached in time.
In Part 4 of the Frailty Paradox series, we explore how signals of deterioration are used to prioritise risk and target coordinated care.